What is the nerve supply to the flexor muscles of the forearm?
View answer
All muscles in the anterior (flexor) compartment are supplied by the median nerve with the exception of flexor carpi ulnaris and flexor digitorum profundus to the little and ring fingers.
Note: The deep group of muscles are supplied by the anterior interosseous nerve which is a branch of the median nerve.
Where do the lumbrical muscles originate and insert?
"
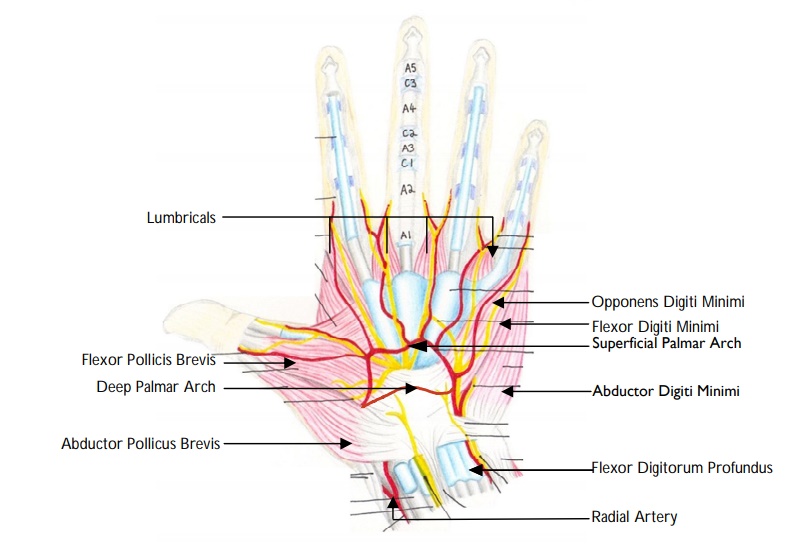
The lumbrical muscles arise from the radial aspect of the FDP tendons in the palm. They insert into the extensor expansions on the dorsum of the digits near the MCPJs.
Note: Therefore the lumbricals flex the digits at the MCPJs and extend the interphalangeal joints.
"
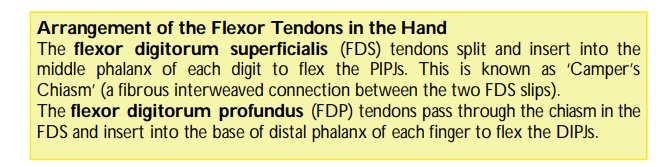
Describe how you would test the function of the flexor digitorum superficialis (FDS) tendon.
"The FDS tendon produces flexion at the proximal interphalangeal joints (PIPJs). It is tested by blocking the finger MCP joint in extension and asking the patient to flex the PIP joint.
"
Describe how you would test the function of the flexor digitorum profundus (FDP) tendon.
"The FDP tendon produces flexion at the distal interphalangeal joints (DIPJs). It is tested by blocking the finger PIP joint in extension and asking the patient to flex the DIP joint.
"
Name the tendon that flexes the interphalangeal joint of the thumb.
"The flexor pollicis longus is the only tendon that flexes the interphalangeal joint of the thumb. It can be tested by holding the proximal phalanx of the thumb and asking the patient to flex the distal interphalangeal joint."
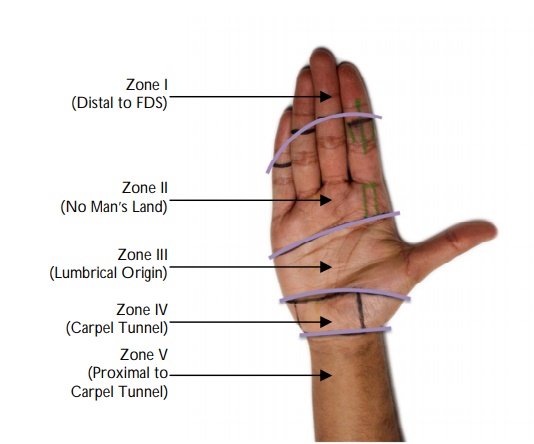
Describe the zones of flexor tendon injuries.
Zone I : Distal to the insertion of FDS.
Zone II : FDS insertion to proximal end of A1 pulley.
Zone III : Mid-palm (from the proximal aspect of the A1 pulley to the distal end of flexor retinaculum).
Zone IV : Under the flexor retinaculum (transverse carpal ligament).
Zone V : From the proximal end of flexor retinaculum (corresponds to distal wrist crease) to the forearm.
Note: Zone II injuries are often referred to as ‘No Man’s Land’ because repair in this zone is very difficult.
Describe the function of the pulley system of the digits.
"The pulleys are fascial attachments to the phalanges which allow the finger to flex and help to prevent bowstringing of tendons. Destruction of this pulley system reduces flexor tendon glide and allows bowstringing which diminishes the excursion and power of the tendons.
"
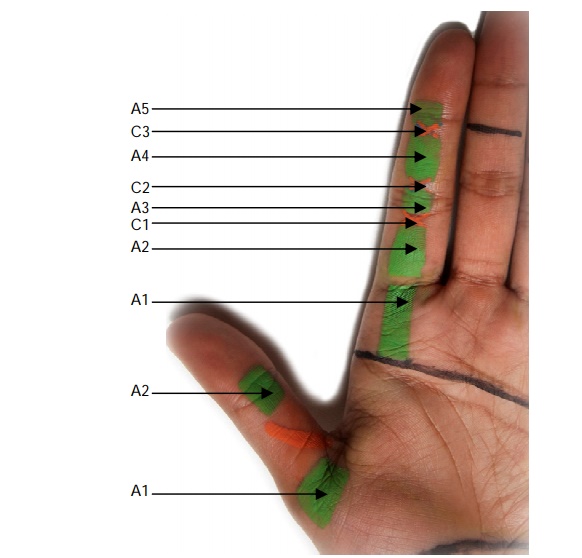
Describe the arrangement of the pulley system in the digits.
The flexor tendons run in a fibrous sheath which is constructed of segments of thickened fibrous solid tunnels (known as annular pulleys) and interlinking collapsible areas (known as cruciate pulleys). The annular pulleys are found over the shafts of the phalanges and the cruciate pulleys over the joints:
A1 : Over the MCPJ.
A2 : Over the proximal phalanx.
C1 : Between A2 and A3.
A3 : Over the PIPJ.
C2 : Between A3 and A4.
A4 : Over middle phalanx.
C3 : Between A4 and A5.
A5 : Over the DIPJ.
Note: The pulley’s often referred to as the ‘critical pulleys’ (as they prevent bowstringing) are the annular pulleys, particularly A2 and A4.
Describe the ‘Jersey-finger’ type tendon injury.
"Traumatic FDP avulsion from the tendon-bone junction at its insertion to the distal phalanx can occur following hyperextension of the distal interphalangeal joint (DIPJ) which subjects the FDP tendon to an excessive load. This is commonly seen in athletes such as rugby players. When one player grabs another’s jersey a finger may be caught and pulled, resulting in disruption of the flexor tendons (‘jersey finger’). This type of injury is most commonly seen in the ring finger.
"
Name the tendon in the forearm that is most commonly used for reconstruction.
"
Palmaris longus (absent in approximately 10-15% of the population) can be harvested for a tendon graft and is often used for reconstruction.
Note: It ends in the fan-shaped palmar fascia.
"
Describe the layers of the palmar fascia.
"
The palmar aponeurosis (palmar fascia) is made up of three layers:
- A superficial layer containing longitudinal fibres.
- An intermediate layers containing transverse fibres.
- A deep layer containing vertical fibres.
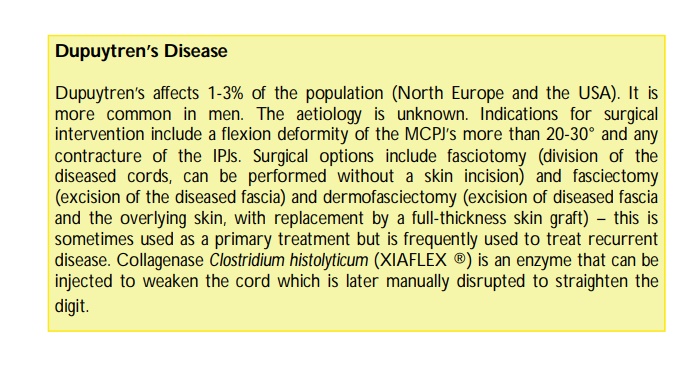
What is Dupuytren’s disease?
"Dupuytren’s disease is a condition of unknown aetiology characterised by contraction of the longitudinal fibres of the palmar or digital fascia.
"
Which digits does Dupuytren’s most commonly affected?
Dupuytren’s disease most commonly affects the ring and little fingers.
What other fibromatous conditions are associated with Dupuytren’s disease?
Conditions associated with Dupuytren’s disease include:
Garrod’s pads: knuckle pads.
Peyronie’s disease: penile fibrous plaques.
Ledderhosen’s disease: plantar fibromatosis.
What is a trigger finger?
"Trigger finger, also known as stenosing tenosynovitis, is due to a mismatch between a thickened or stenotic first annular (A1) pulley in the hand and the flexor tendon trying to glide through the pulley. This causes the flexor tendon to catch or lock proximal interphalangeal joint as the patient attempts to extend the finger, results in difficulty flexing or extending the finger known as the ‘triggering’ phenomenon.
"