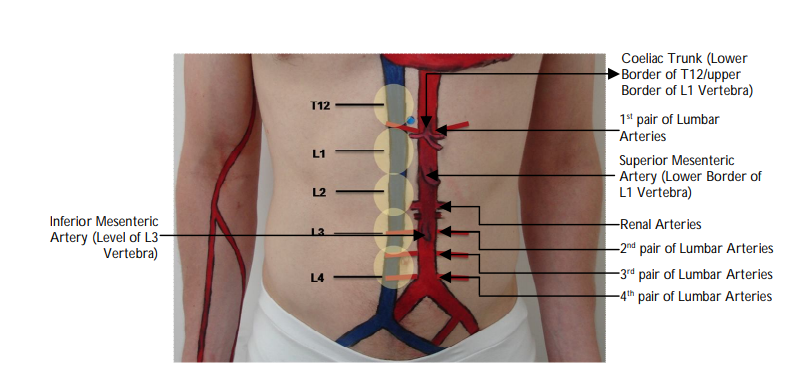
At what vertebral level does the abdominal aorta bifurcate?
"The aorta bifurcates at the lower border of L4 vertebra.
"
Name the anterior unpaired branches of the abdominal aorta.
"
The sub-diaphragmatic unpaired anterior branches of the abdominal aorta are:
- Coeliac trunk
- Superior mesenteric artery (SMA)
- Inferior mesenteric artery (IMA)
At what vertebral level does the coeliac trunk arise.
"The coeliac trunk arises at the lower border T12/upper border of L1 vertebra, originating just distal to the aortic hiatus of the diaphragm.
"
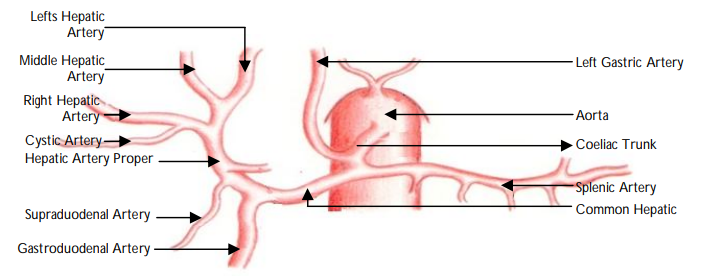
Name the major branches of the coeliac trunk.
The major branches of the coeliac trunk are the Left gastric artery, common Hepatic artery and Splenic artery.
Which visceral organs do the branches of the coeliac trunk supply?
The coeliac trunk supplies adult structures derived from the foregut (from the mesoderm): abdominal oesophagus, liver, gallbladder, spleen, stomach, proximal duodenum (up to second part) and some portion of the pancreas.
At what vertebral level does the superior mesenteric artery arise?
"The SMA arises at the level of the lower border of L1 vertebra.
"
Name the branches of the superior mesenteric artery.
"
The major branches of the SMA are:
- Inferior pancreatico-duodenal arteries.
- Intestinal (jejunal and ileal branches).
- Ileocolic arteries.
- Right colic.
- Middle colic.
Which structures are supplied by the branches of the superior mesenteric artery?
"
Branches of the SMA supply adult derivatives of the midgut. These are:
- Distal to the 2nd part of the duodenum.
- Duodeno-jejunal flexure.
- Head of the pancreas.
- Jejunum.
- Ileum.
- Caecum.
- Appendix.
- Ascending colon.
- Up to the junction of the proximal 2/3rd and distal 1/3rd of the transverse colon.
"At what vertebral level does the inferior mesenteric artery arise? "
"The IMA arises at the level of the lower border of L3 vertebra.
"
Name the major branches of the inferior mesenteric artery.
"
The major branches of the IMA are the:
- Left colic artery.
- Sigmoidal artery.
- Superior rectal artery.
Which structures are supplied by branches of the inferior mesenteric artery?
"Branches of the IMA supply derivatives of the hindgut - the distal 1/3rd of the transverse colon, descending and sigmoid colon and superior rectum.
"
At what vertebral level do the paired renal arteries arise?
The renal arteries arise at the level of L2 vertebra, inferior to the origin of the
SMA
Name the paired arteries of the abdominal aorta
The paired arteries of the abdominal aorta are the:
Inferior phrenic
Middle suprarenal
Gonadal (testicular or ovarian)
Renal
What is an arterial aneurysm?
"An aneurysm is an abnormal dilatation (usually 1.5 x dilatation) of an artery.
"
How do you define a true and a false aneurysm?
"
- A true aneurysm is characterised by dilatation of all layers of the arterial wall (intima, media and adventitia).
- A false aneurysm is characterised by a breach in the vessel wall and the blood is contained by the adventitia or surrounding perivascular tissue. Importantly, a direct communication exists between the vessel lumen and the aneurysm, resulting in a higher risk of rupture than a true aneurysm.
What are the indications for elective repair of an abdominal aortic aneurysm?
"
Current guidelines* recommend elective surgery for patients with aneurysms ≥5.5 cm in diameter and with aneurysms ≥4.5 cm in diameter that have increased by more than 0.5 cm in the past six months. Patients with symptomatic aneurysms of <4.5 cm in diameter should be followed up with USS every six months, and aneurysms 4.5–5.5 cm in diameter should be followed up every three to six months.
* NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Guideline scope. Abdominal aortic aneurysm: diagnosis and management. 2017.
"
Describe how abdominal aortic aneurysms can be anatomically classified.
"
Abdominal aortic aneurysms can be described by their relationship to the renal arteries:
- They are described as supra-renal, juxta-renal, or infra-renal.
- They may extend proximally (forming thoraco-abdominal aneurysms), or distally into the iliac arteries.
- They can also be classified according to shape as saccular or fusiform.
What are the common interventional options for abdominal aortic aneurysm repair?
"Options for abdominal aortic aneurysm repair include open or endovascular. The decision to intervene and the modality is dependent on a number of factors such as the age of the patient, co-morbidities and the anatomical location of the aneurysm (supra-renal, juxta-renal or infra-renal).
"