Identify the points on the image
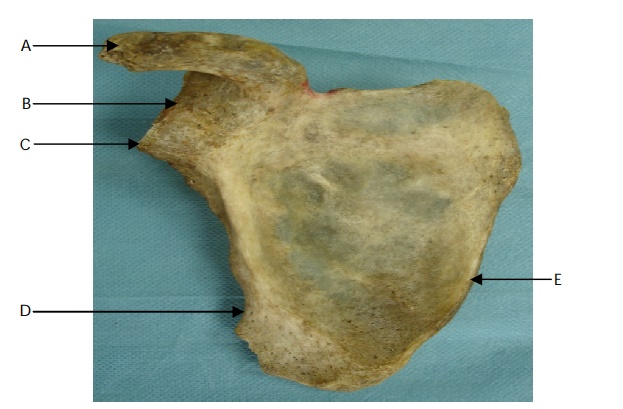
View answer

Which nerve supplies serratus anterior?
"The long thoracic nerve supplies serratus anterior.
"
How does injury to the long thoracic nerve present?
"Injury to the long thoracic nerve presents with winging of the scapula.
"
Name the muscles which attach to the coracoid process.
"
- Coracobrachialis (origin).
- Short head of biceps (origin).
- Pectoralis minor (insertion).
Why is the surface anatomy of the coracoid process an important surgical anatomical landmark?
"
- umeral joint is one finger breadth lateral to coracoid process.
- Attachment of coracoid muscles separates the safe lateral side from medial side (where brachial plexus and vessels lie).
- Clavipectoral fascia covers the floor of deltopectoral groove. Can be identified by internally rotating humerus allowing subscapularis to be identified.
Name the joints that make up the shoulder joint?
"The joints of the shoulder are the glenohumeral joint and the acromioclavicular joint. The clavicle also articulates with the sternum at the sternoclavicular joint.
"
Name the muscles that make up the rotator cuff and their Innervations.
"
- Supraspinatus : Suprascapular nerve (C5, C6)
- Infraspinatus : Suprascapular nerve (C5, C6)
- Teres minor : Axillary nerve (C5, C6)
- Subscapularis : Upper and Lower Subscapular nerves (C5, C6)
Describe the blood supply to the rotator cuff.
"
The blood supply to the rotator cuff is derived from the following arteries:
- Anterior circumflex humeral artery : Supplies anterior cuff & long head of biceps.
- Posterior circumflex humeral artery : Supplies posterior cuff.
- Suprascapular artery : Supplies posterior cuff.
- Thoracoacromial arteries : Supplies supraspinatus.
- Subscapular artery : Supplies subscapularis and infraspinatus.
Which muscles are responsible for abduction at the shoulder?
"
The range of abduction can be divided into 3 parts:
- Initiation of abduction from 0 - 30 degrees: Supraspinatus
- Once initiated, from 30 – 100 degrees: Lateral fibres of deltoid
- Beyond 100 degrees to full abduction: Rotation of the scapula on the thoracic wall aided by trapezius, serratus anterior and levator scapula.
Name some common causes of shoulder pain.
"
- Supraspinatus tendinitis.
- Impingement syndrome.
- Rotator cuff tears.
- Frozen shoulder.
- Calcific tendonitis.
- Subacromial bursitis.
What are the symptoms of 'painful arc syndrome'?
 "Painful arc syndrome is also synonymous with 'shoulder impingement syndrome' or 'subacromial impingement'. Supraspinatus tendinitis is the most common cause. Other aetiologies include: subacromial spurs, osteoarthritic spurs on the AC joint, calcification of the coraco acromial ligament and subacromial bursitis. Symptoms include pain and weakness abduction during abduction between 60 and 120 degrees when the inflamed tendon is compressed against the acromion. Outside this range, abduction is usually pain-free.
"
"Painful arc syndrome is also synonymous with 'shoulder impingement syndrome' or 'subacromial impingement'. Supraspinatus tendinitis is the most common cause. Other aetiologies include: subacromial spurs, osteoarthritic spurs on the AC joint, calcification of the coraco acromial ligament and subacromial bursitis. Symptoms include pain and weakness abduction during abduction between 60 and 120 degrees when the inflamed tendon is compressed against the acromion. Outside this range, abduction is usually pain-free.
"
Describe the different types of dislocations of the shoulder joint.
Anterior dislocations:
Ninety-five per cent of shoulder dislocations are anterior. In most cases, the head of the humerus comes to rest under the coracoid process, known as sub-coracoid dislocation. The other anterior subtypes include sub-glenoid and sub-clavicular.
Most common causes include a direct blow or a fall on an outstretched arm. In an anterior dislocation, the arm is held in slight abduction and external rotation. There is loss of the rounded muscular appearance of the shoulder and the appearance of a surface depression distal to the acromion resulting from displacement of the humeral head.
Posterior dislocations:
Posterior shoulder dislocations are rare (<5%) and usually seen following seizures or electric shock injuries. Patients present with an adducted and internally rotated arm with flattening of the anterior shoulder and a prominent coracoid process.These dislocations may go unrecognised in unconscious trauma patients or in the elderly. An A-P radiograph shows an internally rotated humeral head which gives a rounded appearance (‘lightbulb sign’). Radiographs may also reveal an increased distance (>6 mm) between the medial border of the humeral head and the anterior glenoid rim (‘rim-sign’).
Note: Inferior dislocations occur in <1% from hyperabduction of the arm which forces the humeral head against the acromion. Such dislocations have a higher rate of injury to the vessels, nerves, tendons and ligaments of the axilla. Likewise, the shoulder may dislocate superiorly (<1%) when the humeral head is driven upwards through the rotator cuff seen in fractures of the humerus, clavicle or acromion.
What are the complications of shoulder dislocation?
The complications that can arise following dislocation of the shoulder include:
• Axillary nerve injury.
• Associated fracture - e.g., of the humeral head, greater tuberosity, acromion or clavicle.
• Bankart lesion - avulsion of the anterior capsulolabral complex from the glenoid rim (seen in anterior dislocation of the shoulder).
• Hill-Sachs lesion - indentation fracture of the posterolateral humeral head (seen in about 40% of anterior dislocations and large proportion of recurrent dislocations).
• Shoulder stiffness.
• Rotator cuff tears.
• Axillary artery injury - rare but may occur with anterior or inferior dislocations in older patients with atherosclerosis.
• Injury to other related nerves in the vicinity such as radial nerve and long thoracic nerve.
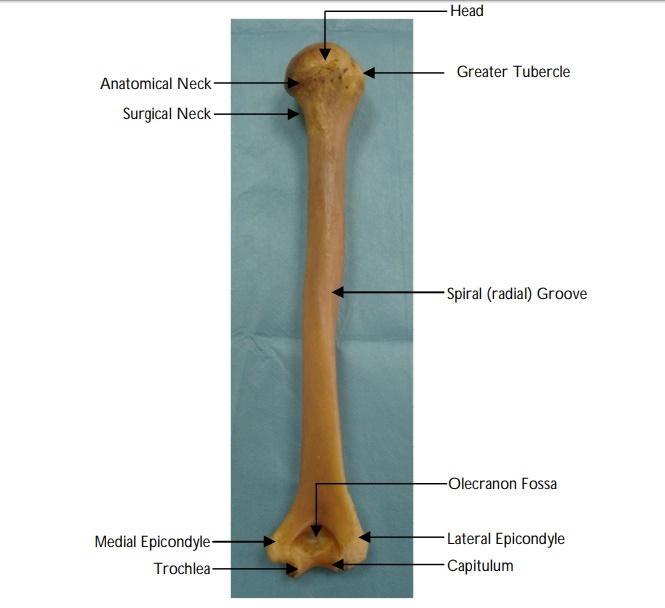
Name the parts of the humerus
Name the muscles that attach to the medial and lateral lips of the intertubercular groove (bicipital grove) of the humerus.
"
- Pectoralis major.
- Latissimus dorsi.
- Teres major.
"Which nerves are susceptible to injury following a fracture of the humerus? "
"
The nerves which are susceptible to injury following a fracture of the humerus are the:
- Axillary nerve : Fractures of the surgical neck of the humerus.
- Radial nerve : Fractures of the shaft of humerus at the junction between the proximal two thirds and distal third (at the level of spiral grove).
- Ulnar nerve : Medial epicondyle fractures.
- Median nerve : Supracondylar fractures.