What is Sibson’s fascia?
"Sibson’s fascia, also known as the suprapleural membrane, attaches to the inner border of the 1st rib and transverse process of C7 vertebra. It is an extension of the endothoracic fascia that exists between the parietal pleura and the thoracic cage and extends approximately 2-2.5 cm above the superior thoracic aperture. It prevents further extension of the lungs and pleura into the neck during inspiration.
"
What important structures lie on the Sibson’s fascia?
"The subclavian artery, subclavian vein and brachial plexus lie on the Sibson’s fascia.
"
Name the important structures within the root of the neck.
"
The root of the neck is the junction between the neck and thorax and contains all structures passing between the neck and thorax:
- Arteries: Common carotid (right and left), subclavian arteries (right and left)
- Veins: Right and left IJV and subclavian veins forming the (right and left brachiocephalic veins).
- Trachea
- Oesophagus
- Vagus nerves
- Phrenic nerves
- Thymus gland
What is the stellate ganglion?
"The stellate ganglion, also known as the cervicothoracic ganglion, is a sympathetic ganglion formed by the fusion of the inferior cervical ganglion and the first thoracic ganglion located at the level of C7 vertebra.
"
What are the anatomical relations of the stellate ganglion?
"
The stellate ganglion:
- Lies anterior to the transverse process of C7.
- Superior to the neck of the 1st rib.
- Just below the subclavian artery.
- The vertebral artery lies anterior to the ganglion as it has just originated from the subclavian artery.
What is the clinical significance of the stellate ganglion?
"
- Excision of the ganglion (sympathectomy) is performed to minimise symptoms associated with Raynaud’s phenomenon, hyperhidrosis (specifically in palmar hyperhidrosis) and facial blushing. This is usually performed endoscopically.
- Local anaesthetic block (stellate ganglion block) can be performed by injecting near the stellate ganglion to minimise sympathetically medicated pain such as complex regional pain syndrome.
Describe the origin and termination of the internal jugular vein.
"
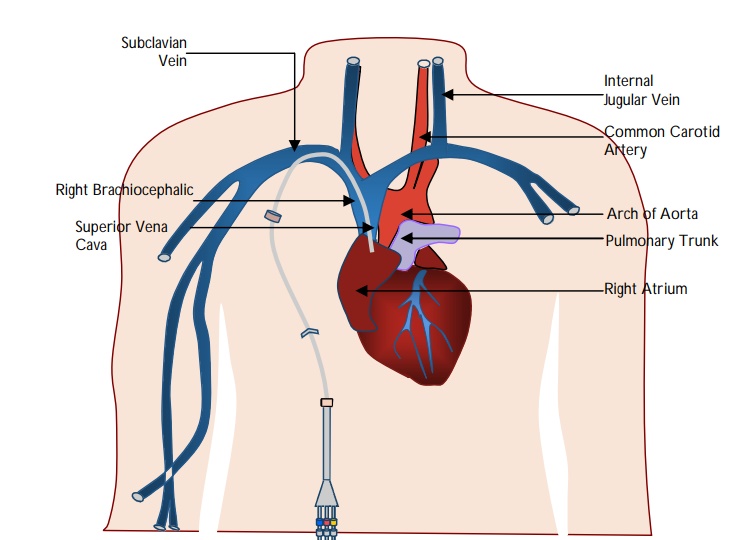
- The inferior petrosal sinus and the sigmoid sinus join at the base of the brain to form the internal jugular vein (IJV) and exits the skull through the jugular foramen.
- The right and left IJV unites with the corresponding subclavian vein to form the brachiocephalic vein.
- The right and the left brachiocephalic veins unite to form the superior vena cava.
How would you identify the internal jugular vein when performing central venous line cannulation via the high approach?
"
- The IJV lies in the anterior triangle of the neck.
- The carotid sheath lies just in front of the anterior border of sternocleidomastoid muscle (SCM)
- The IJV may lies within the carotid sheath (along with the internal carotid artery and vagus nerve).
- The carotid artery lies anteromedially within the sheath.
Note: The needle should be inserted pointing towards the ipsilateral nipple. The carotid artery should be identified and gently moved medially to avoid inadvertent cannulation.
"
How would you identify the internal jugular vein when performing central venous line cannulation via the low approach?
"
- The IJV lies lateral and inferior to the junction of the sternal and clavicular heads of sternocleidomastoid.
- The pleura lies inferomedial and the subclavian artery lies lateral to the IJV.
- The IJV drains into the brachiocephalic vein. On the right this is shorter and drains more vertically into the superior vena cava (therefore making it easier to cannulate).
Which structure lies between the internal jugular vein and carotid artery.
The vagus nerve lies between the internal jugular vein and the carotid artery in the neck.
Describe the approach to cannulation of the subclavian vein
The subclavian vein can be identified as it follows the course of the subclavian artery in the neck, curving laterally over the apex of the lung to reach the 1st rib.
The subclavian vein lies anterior to insertion of scalenus anterior on the first rib (artery lies posterior).
The needle is advanced initially at the junction of the outer and middle 1/3rd of the clavicle at 45°, then directed towards the suprasternal notch.
Name some indications for insertion of a central venous catheter.
"
Indications for insertion of a central venous catheter include:
- Frequent or persistent requirement for intravenous access.
- Long term intravenous fluids and drug administration.
- For patients requiring frequent blood monitoring.
- Chemotherapy/administration of drugs prone to be toxic to peripheral veins (e.g., vasopressors).
- Haemodialysis/ haemofiltration.
- Monitoring of the central venous pressure (CVP).
Name the potential complications of internal jugular vein cannulation.
Complications of insertion of internal jugular vein cannulation include:
Immediate:
Injury to local structures resulting in:
Bleeding (risk of significant haemorrhage from the carotid artery).
Pseudoaneurysm.
Pneumothorax.
Haemothorax.
Chylothorax (specifically on the left side due to presence of the thoracic duct).
Nerve injuries (in particular brachial plexus and vagus nerve).
Cardiac arrhythmias.
Air embolism.
Retention of guide wire.
Late:
Sepsis.
Thromboembolism.
AV fistula formation.