View answer
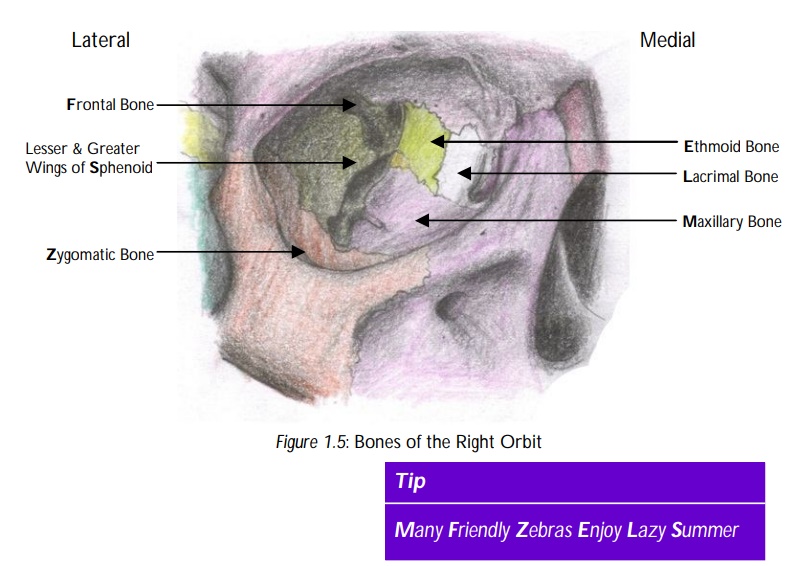
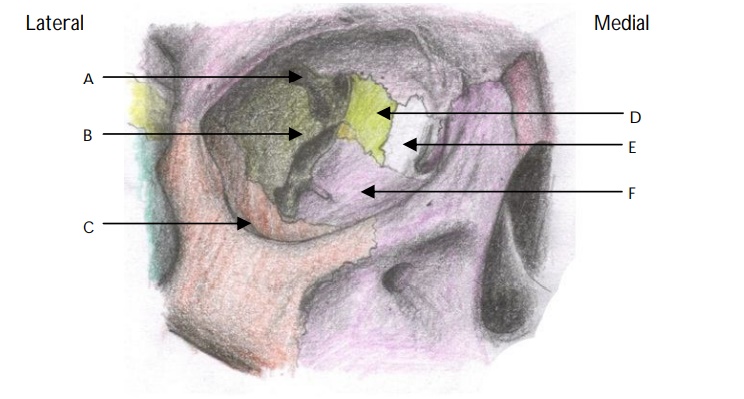
Name the openings within the orbit.
"
- Superior orbital fissure.
- Inferior orbital fissure.
- Anterior ethmoid foramen.
- Posterior ethmoid foramen.
- Optic canal.
Name the structures which pass through the superior orbital fissure.
"
Structures passing through the superior orbital fissure are the:
- Superior ophthalmic vein
- Inferior opthalmic vein
- Ophthalmic division of trigeminal nerve and its branches (lacrimal, frontal and nasociliary)
- CN III - Occulomotor nerve (Superior and Inferior Divisions)
- CN IV - Trochlear nerve
- CN VI - Abducens nerve
- Sympathetic nerve fibres
Name the structures that pass through the inferior orbital fissure.
"
Structures passing through the inferior orbital fissure are the:
- Infraorbital nerve
- Zygomatic nerve
- Infraorbital artery
- Infraorbital veins
- Inferior ophthalmic vein
Name the structures that pass through the anterior and posterior ethmoid foramina.
"
Structures passing through the anterior ethmoid foramen are the:
- Anterior ethmoid nerve
- Anterior ethmoid vessels
Structures passing through the posterior ethmoid foramen are the:
- Posterior ethmoid nerve
- Posterior ethmoid vessels
Name the structures that pass through the optic canal.
"
Structures passing through the optic canal are the :
- Optic nerve (with meninges and CSF)
- Ophthalmic artery
- Central retinal vein
- Central retinal artery
"What is the functional loss due to an abducens nerve palsy? "
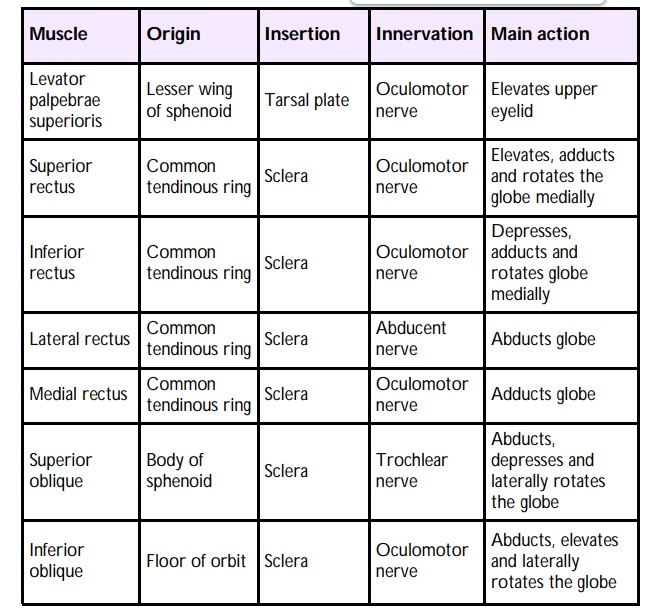
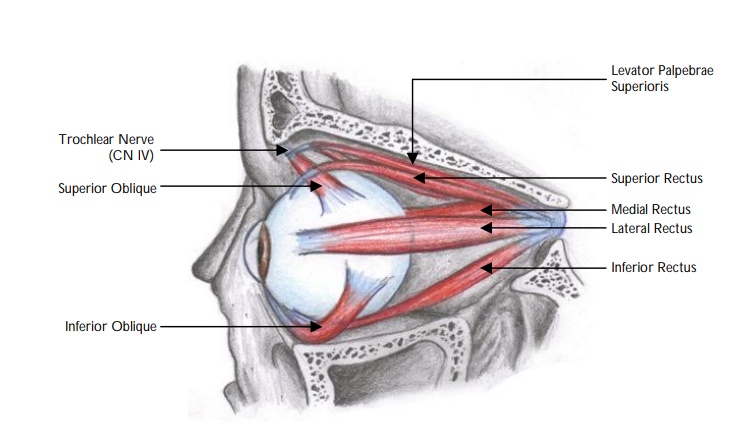
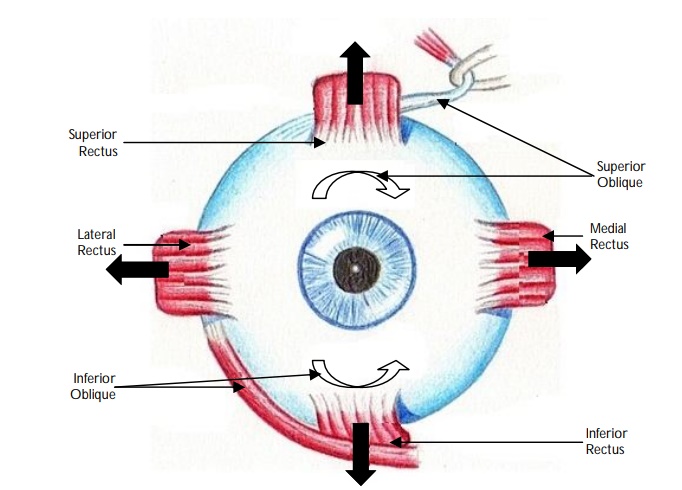
In abducens nerve palsy, the lateral rectus is no longer able to abduct the eye causing convergent strabismus.
What is the functional loss due to an occulomotor nerve palsy?
An occulomotor nerve palsy will result in loss of function of the levator palpebrae superioris; inferior oblique, medial, superior and inferior recti muscles and the sphincter pupillae muscle. The eye has a characteristic ‘down and out’ position as well as ptosis (drooping of the eyelid) and mydriasis (pupil dilation). The pupillary dilatation is caused by the denervation of the parasympathetic fibres that are carried along with the occulomotor nerve.
What is the functional loss due to a trochlear nerve palsy?
A trochlear nerve palsy will result in paralysis of the superior oblique muscle. The affected eye has a characteristic upwards and inwards position and patient may present with diplopia.
Note: Patients may find head tilting a good compensatory position.
What is orbital cellulitis?
Orbital cellulitis refers to inflammation affecting the tissues around the eye. Orbital cellulitis may be pre-septal or post-septal depending on its relationship to the orbital septum. It is usually associated with a sinusitus, local soft tissue infection or following trauma to the face and URTI.
What is the management of orbital cellulitis?
The patient is treated aggressively with intravenous antibiotics and nasal decongestants. Any abscess should be drained urgently to minimise the risk of visual compromise.
Name two complications of orbital cellulitis.
Infections behind the septum of the eye can result in an abscess resulting in visual compromise. Rarely the infection can spread intra-cranially causing a cavernous sinus thrombosis.