LOWER LIMB
OSCE
Station 5
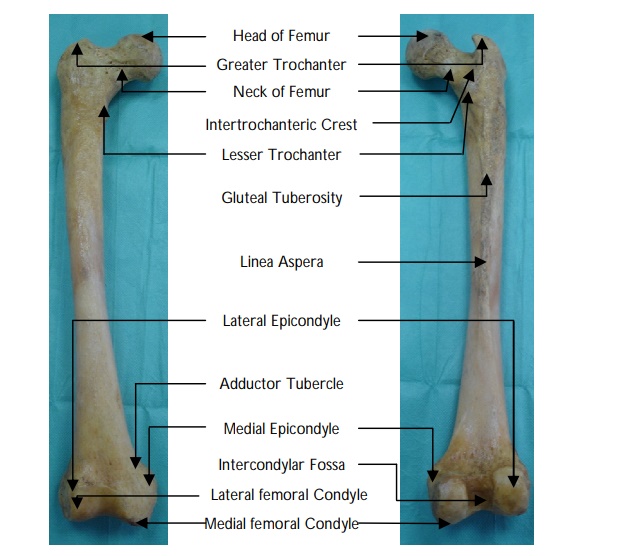
Femur and high
Identify the labels on the image:

View answer
What are the stages of ossification of the proximal femur?
"
The proximal end of the femur can be divided into five ossification centres:
- Femoral shaft: Undergoes ossification at 7 weeks in utero.
- Femoral capital epiphyses: Undergoes ossification at 2-4 months in utero.
- Femoral head: Undergoes ossification at 4-6 months of age.
- The greater trochanter: Undergoes ossification at 2-4 years of age
- The lesser trochanter: Undergoes ossification at puberty.
Note: All of femoral ossification centres fuse between the ages of 14 and 18.
"
Briefly describe ‘Coxa Vara’ and ‘Coxa Valga’
"The angle of inclination that the long axis of the femoral head makes with the femoral body varies with sex, age, disruption of congenital development and pathological processes that may weaken the neck of the femur such as rickets. When the angle of inclination is decreased, this is known as Coxa Vara; when it is increased it is known as Coxa Valga. Coxa Vara results in a shortening of the lower limb and can limit passive abduction of the hip.
"
How can fractures of the femoral neck be classified?
"
- Fractures of the femoral neck can be broadly classified into intra-capsular and extra-capsular fractures.
- Intra-capsular fractures are more prone to avascular necrosis due to the nature of the blood supply and limited surface area for bony union whilst extra-capsular fractures do not pose this risk.
- Extra-capsular fractures are further subdivided based on their location into per-trochanteric, intra-trochanteric and sub-trochanteric fractures.
- Basal fractures occur at the junction between the intra and extra-capsular division.
- The management of intra and extra-capsular fractures are fundamentally different due to the nature of the blood supply, surface area available for bony union and dynamics of the hip joint.
Describe the Garden classification of intracapsular fractures of the femoral neck.
"
The Garden classification grades all intracapsular fractures of the femoral neck. Types I and II are undisplaced whilst types III and IV are displaced fractures:
- Type 1 : Undisplaced, incomplete or impacted fracture.
- Type II : Undisplaced, complete fracture.
- Type III : Complete fracture with partial displacement.
- Type IV : Complete fracture with total displacement.
Describe how you would manage an intracapsular fracture of the hip.
"
- Garden types I and II are usually managed by internal fixation with cannulated hip screws (AO screws) or can be managed conservatively (if the patient is not fit for surgery).
- Garden types III and IV generally require arthroplasty (hemiarthroplasty in the majority of elderly patients, however younger patients may require total hip replacement). In young patients with Garden type III fracture, sometimes AO screw fixation can be attempted with the aim of salvaging the femoral head.
"
Describe the management of extracapsular fractures.
"Extra-capsular hip fractures do not pose a threat to the blood supply to the femoral head and there is a larger surface area for bony union when compared with intra-capsular fractures. Stable extra-capsular fractures are usually managed with a Dynamic Hip Screw (DHS). Fractures below the sub-trochanteric level
(> 5 cm below the lesser trochanter) may require intra-medullary nailing. Grossly contaminated or comminuted fractures may require external fixation."
Name the muscles that make up the ‘true hamstrings’ and their innervation.
"
- The true hamstrings are those muscles that cross both the hip joint and the knee joint and are extensors of the thigh and flexors of the leg. These muscles are the:
- Semitendinosus.
- Semitendinosus.
- Long head of biceps femoris.
- The short head of biceps femoris is frequently considered as part of the hamstrings although it does not meet the above criteria. Whilst the true hamstrings arise from the ischial tuberosity, the short head of biceps femoris arises from the linea aspera and lateral supracondylar line of the femur.
- Whilst the true hamstring muscles are innervated by the sciatic nerve, specifically the tibial division (L5, S1 and S2), the short head of biceps is frequently innervated by the common peroneal division of the sciatic nerve.
Describe the function of the hamstring muscles.
"
The hamstrings cross the hip and knee joints. They are extensors of the thigh and flexors of the leg. They play a crucial role in many daily activities, such as, walking, running and jumping. In walking, they act as an antagonist to the quadriceps in the deceleration of knee extension.
- Semitendinosus and semimembranosus:
- They medially rotate the lower leg when the knee is flexed; can also help to extend the hip when the trunk is fixed.
- Biceps femoris:
- The long head of the biceps femoris extends the hip (such as when beginning to walk); both short and long heads flex the knee and laterally rotates the lower leg when the knee is flexed.
How would you clinically test the function of the hamstrings?
"To test the function of the hamstrings flex the patient’s leg against resistance whilst palpating their tendons on each side of the popliteal fossa (which should feel prominent as the patient flexes their knee).
"
Name the adductor muscles of the thigh.
"
The adductor muscles of the thigh are the:
- Adductor longus.
- Adductor brevis.
- Adductor magnus.
- Gracilis.
Name the nerve supply to the medial (adductor) compartment of the thigh.
The obturator nerve (L2, 3, 4) supplies the medial compartment of the thigh. The hamstring part of adductor magnus is also supplied by the tibial part of the sciatic nerve.
Name the muscles which make up the quadriceps
The muscles that make up the quadriceps are the:
Rectus femoris.
Vastus lateralis.
Vastus medialis.
Vastus intermedius.
What is the innervation of the quadriceps femoris?
The femoral nerve (L2, 3, 4) innervates the quadriceps femoris
What is the Hunter’s canal?
"
- The Hunter’s canal (also known as the subsartorial or adductor canal) is an aponeurotic sheath in the thigh located in the middle 1/3rd of the antero-medial part of the thigh.
- It lies deep to the middle third of sartorius extending from the apex of the femoral triangle to the adductor hiatus (opening in the adductor magnus). The canal provides an intermuscular passage through which the femoral vessels pass to reach the popliteal fossa.
Name the boundaries of the Hunter’s canal.
"
- Lateral : Vastus medialis.
- Posterior : Adductor longus and adductor magnus.
- Anterior : Sartorius.
Name the contents of the Hunter’s canal.
"
The contents of the Hunter's canal are the:
- Superficial femoral artery.
- Femoral vein.
- Saphenous nerve.
- Nerve to vastus medialis.
- Terminal division of the obturator nerve.
- Deep lymphatics.
Note: The nerves do not exit through the Hunter’s canal. The saphenous nerve perforates the gracilis and sartorius to run in the superficial fascia along with the long saphenous vein. The nerve to vastus medialis lies in the Hunter’s canal where it supplies vastus medialis but does not exit the canal.
"