Describe the course of the oesophagus.
"
The oesophagus:
- Is normally 18-25 cm long.
- Is continuous with the laryngopharynx and begins at the level of the inferior border of the cricoid cartilage at the level of C6 vertebrae.
- Descends through the left side of the superior mediastinum and then enters the posterior mediastinum (behind the trachea and the heart) before passing through the diaphragm at T10 vertebral level.
- Enters the cardia of the stomach.
Where are the constrictions of the oesophagus?
"
The oesophagus has 3 constrictions in its vertical course:
1st constriction : Approximately 15 cm from the upper incisor teeth, where the oesophagus commences at the cricopharyngeal sphincter; this is the narrowest portion of the oesophagus and approximately corresponds to C6 vertebra.
2nd Constriction : Approximately 23 cm from the upper incisor teeth, where it is crossed by the aortic arch and left main bronchus.
3rd Constriction : Approximately 40 cm from the upper incisor teeth, where it pierces the diaphragm; at the level of the lower oesophageal sphincter.
Note: These measurements are clinically important since these are the sites where foreign bodies can be impacted. They are also important for endoscopy and endoscopic surgery.
"
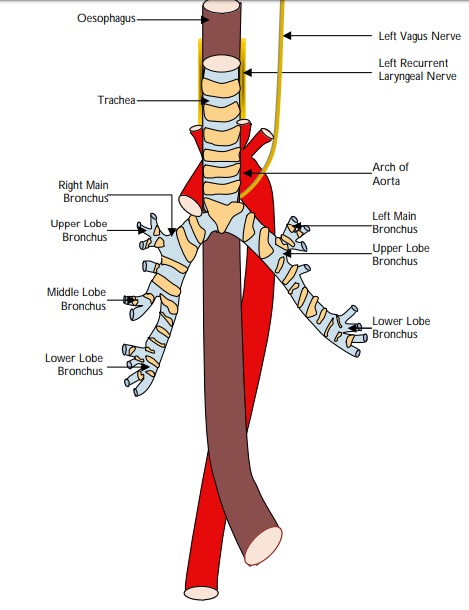
Name the nerve that lies on either side of oesophagus.
"The recurrent laryngeal nerves lie in the tracheo-oesophageal grooves on either sides of the oesophagus.
"
How is the oesophagus anatomically divided?
"
The oesophagus can be divided into:
- Upper, middle and lower thirds or into cervical, thoracic, abdominal parts.
What is the arterial supply of the oesophagus?
"
The arterial supply of the oesophagus is segmental:
- Cervical part : Inferior thyroid branch of thyrocervical trunk (from subclavian artery).
- Thoracic part : Branches from the descending thoracic aorta and bronchial arteries.
- Abdominal part : Oesophageal branch of left gastric artery and inferior phrenic artery.
Describe the venous drainage of the oesophagus.
"
The venous drainage of the oesophagus is again segmental:
- Cervical part : Inferior thyroid veins.
- Thoracic part : Azygos, hemiazygos and accessory azygos veins.
- Abdominal part : Azygos and left gastric vein (the left gastric is a tributary of the portal vein therefore this is a site of porto-systemic anastamosis).
Describe the innervation of the oesophagus.
"
The innervation of the oesophagus is:
- Cervical part : Recurrent laryngeal nerves (somatic fibres) and cervical sympathetic trunks (vasomotor fibres).
- Thoracic part : Branches from vagal trunks, oesophageal plexus, sympathetic trunks and greater splanchnic nerves.
- Abdominal part : Vagal trunks (anterior and posterior gastric nerves), thoracic sympathetic trunks, greater and sometimes lesser splanchnic nerves, and plexuses around left gastric and inferior phrenic plexuses.
"
Describe the musculature of the oesophagus.
"
The musculature of the oesophagus is arranged in two planes - external longitudinal fibres and internal circular fibres. The muscle changes from voluntary skeletal muscle to involuntary smooth muscle as the oesophagus travels inferiorly from pharynx to the stomach:
- Upper third : Striated muscle.
- Middle third : Mixture of striated and smooth.
- Lower third : Smooth muscle.
What is Barrett’s oesophagus?
"Barrrett’s oesophagus is a metaplastic change occurring at the lower end of the oesophagus. This occurs when any portion of the normal distal squamous epithelial lining gets replaced by metaplastic columnar epithelium due to sustained reflux disease.
"
"Name some potential causes for oesophageal perforation. "
"
Some potential causes for oesophageal perforation include:
- Spontaneous rupture, usually a tear just above the cardia, on the left wall of the oesophagus:
The classical presentation is Boerhaave’s syndrome, with patients complaining of severe chest/abdominal pain following an episode of vomiting.
- Penetrating injury (rare).
- Iatrogenic perforation (i.e., during endoscopic procedures).
"