Describe the course of the ureter.
"
The ureter can be divided into three parts; abdominal, pelvic and intravesical:
- Arises at the proximal expanded renal pelvis.
- Runs vertically downwards along the edges of the transverse processes of L1-L5 vertebrae towards the sacroiliac joint.
- Enters the pelvis anterior to the sacroiliac joint at the bifurcation of the common iliac vessels (at the pelvic brim) and then courses anterior to the internal iliac artery down the lateral pelvic sidewall.
- At the level of the ischial spine, it turns forward and medially to enter the posterolateral wall of the bladder, where it runs an oblique 1-2 cm course, before opening into the bladder at the internal ureteric orifice.
Name the vessel that crosses the ureter as it enters the pelvic brim.
"The ureter crosses the external iliac artery just distal to the bifurcation of the common iliac artery.
"
Describe the relationship of the ureter to the uterine artery in the female pelvis.
"
The ureter passes beneath the uterine artery, lateral to the cervix.
Note: In the male pelvis, the relationship of the ureter to the ductus deferens can be compared to that between the ureter and the uterine artery. The ureter passes inferior to the ductus deferens as the ductus deferens passes along the lateral wall of the pelvis on its course to the seminal vesicle.
"
Describe how you would quickly identify the ureter during intra-abdominal surgery.
"
In order to prevent inadvertent injury to the ureter during abdominal surgery (mainly colectomies and during gynaecological procedures) it is important to recognise and preserve the ureters. They can easily be identified by the key features:
- Course along the sacroiliac joints.
- At the pelvic brim the ureter passes over the bifurcation of the common iliac.
- As it descends further it lies medial to the internal iliac arteries on the posterolateral pelvic side wall.
- Visible peristalsis.
Name the constrictions of the ureter.
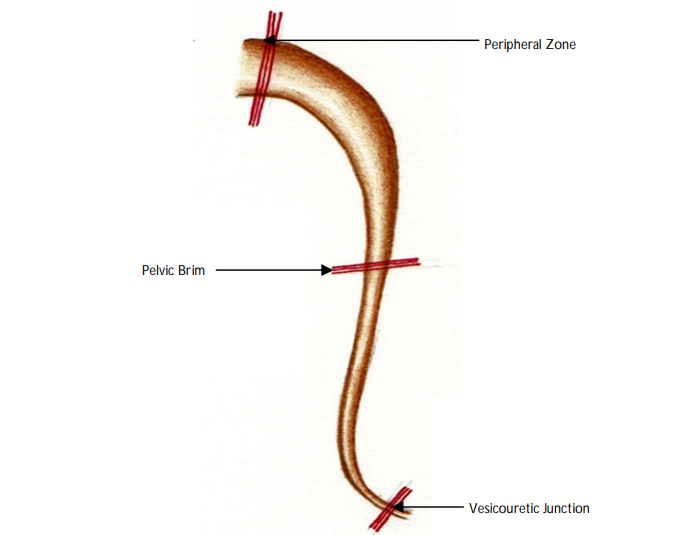
There are three sites of narrowing along the course of the ureter and therefore, sites where a calculus is most likely to lodge:
Pelviureteric junction
Pelvic brim
Vesicoureteric junction
Describe the blood supply to the ureter.
"
The ureters receive a segmental blood supply from 4 main sources:
- Renal arteries
- Gonadal arteries
- Internal iliac arteries
- Superior and inferior vesical arteries
What type of epithelium lines the lumen of the ureter?
"The lumen of the ureter in lined by transitional epithelium.
"
What serious complication can arise following ureteric obstruction?
"Hydronephrosis, distension and dilatation of the renal pelvis and calyces, is the most serious consequence of ureteric obstruction. Drainage of the kidney is usually required, either through a percutaneous nephrostomy or retrograde ureteric stenting.
"
Describe where ureteric calculi may be identified on a plain radiograph of the kidney, ureters and bladder (‘X-ray KUB’).
"
The course of the ureter can be correlated with the bony anatomy visible on a plain radiograph
- Passing inferiorly along the tips of the transverse processes of the vertebral bodies.
- Passing over the sacroiliac joint to the level of the ischial spines then medially into the bladder.
Name the most common type of urinary tract calculus (by composition).
"The most common stone composition is calcium oxalate (around 85% of stones).
"
Name the type of stone (by composition) that is most commonly responsible for staghorn calculi.
"Staghorn calculi are most commonly struvite, but may be formed by other substances such as calcium oxalate or uric acid.
"
Name the radiolucent stone that occurs in acidic urine
Urate stones form in acidic urine, whereas alkaline urine predisposes to the formation of other types of stones.
Other than calculi, name some other causes of unilateral hydronephrosis
Unilateral hydronephrosis can be secondary to pathology other than stone disease, including:
Intrinsic:
Transitional cell carcinoma of the renal pelvis or ureter
Ureteric stricture
Extrinsic:
Tumour e.g., colonic, cervical, prostatic
Abnormal vasculature at the pelviureteric junction
Idiopathic retroperitoneal fibrosis
Post-radiation fibrosis
Abdominal aortic aneurysm